
African swine fever – outbreak in the Caucasus and why Australia should be aware
Recent activity
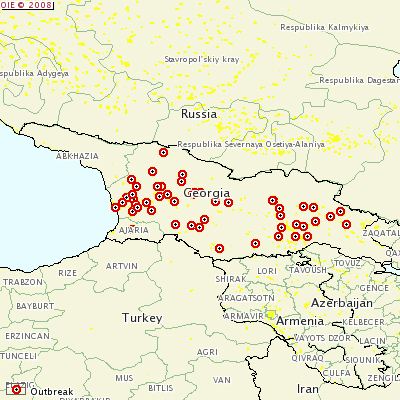
African swine fever (ASF) has usually been restricted to Africa with occasional outbreaks in southern Europe.On 17 May 2007, Georgia reported an outbreak of postweaning multisystemic wasting syndrome due to porcine circovirus type 2. ASF was also suspected in the early stages of the outbreak. However, ASF and classical swine fever (CSF) were ruled out after pathological material from 150 animals was tested in the Georgian Ministry of Agriculture. As the outbreak progressed, Georgia sent samples from affected pigs to the OIE Reference Laboratory in Pirbright, UK where a positive diagnosis of ASF was made on 4 June 2007. Two different locations in Georgia simultaneously first reported the outbreak in April 2007, suggesting the virus had already been present in the country for several weeks.
Over 90% of pigs in Georgia belong to small pig farmers in rural areas with only one to two pigs per farm. There are no slaughter houses so butchering is done on the farm, with only domestic waste disposal arrangements in place. Pigs are allowed to roam free in the villages during the day and have access to waste, including kitchen and slaughter waste. Wild boars inhabit forested areas in the Caucasus and occasionally enter villages while scavenging for food.
According to the Food and Agriculture Organisation of the United Nations (FAO), once the virus was recognised in Georgia, the government adopted a ‘plan of activities against African Swine Fever Virus’, which consisted of 15 actions for the control of ASF. These measures included movement controls of pigs, pork and materials that might spread the infection, confinement, and, culling of free-roaming pigs and cleaning/disinfection of premises. According to the FAO, limited veterinary services, poor biosecurity and swill feeding further complicated disease control in Georgia. Furthermore, often only clinically ill animals in a herd or village were culled, allowing other animals to spread the disease. More problematic was that most cases of ASF were reported based on clinical signs without laboratory confirmation, resulting in incorrect reporting.
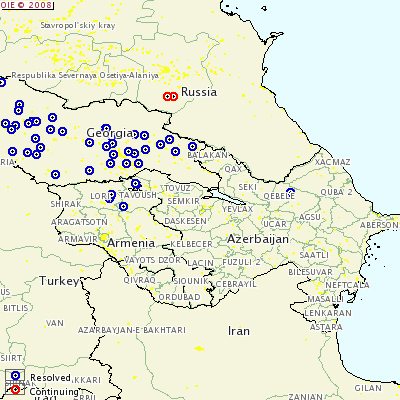
Delayed recognition of the disease, combined with the issues regarding disease control identified above, resulted in ASF becoming widespread in Georgia. By the end of 2007, outbreaks of ASF had been reported in both Armenia and Russia with further spread occurring in 2008 in Russia and Azerbaijan. Outbreaks of ASF are still occurring in the Caucasus.
What’s in a disease?
ASF is a highly contagious and fatal disease with the potential to spread rapidly throughout pig populations by direct or indirect contact. ASF is endemic in most of Sub-Saharan Africa where it affects both commercial and smallholder pig production. The disease often has severe socioeconomic effects on rural farmers as entire herds may be lost in an outbreak.
There is no vaccine or treatment available and the disease can only be controlled through stamping out and strict movement controls.
What clinical signs would you expect to see?
ASF is a highly variable disease and most commonly appears in the acute form as a haemorrhagic fever. The incubation period is generally 5 to 7 days in peracute and acute forms, but it can be as long as 20 days.
Predominantly in the peracute form there is high morbidity and mortality with no prior clinical signs. The whole herd may be affected in only a few days. In the acute form, most commonly there is a high fever, anorexia, lethargy, weakness, recumbency, erythema, and huddling along with a case fatality rate of up to 100%.
Other clinical signs in the acute form can include cyanotic blotching on the ears, tail, lower legs or thigh, abdominal pain, constipation or diarrhoea, generalised haemorrhages in the skin and internal organs, dyspnoea, vomiting, nasal and conjunctival discharges, abortion in sows, and neurological signs including convulsions.
In chronic ASF, the mortality is low although it can be higher in younger animals. There is also a recurrent, transient fever, ill thrift, stunting and emaciation, transient thrombocytopaenia and leukopaenia, pneumonia, arthritis, cutaneous ulcers and death from secondary bacterial infections. Pigs may also become chronic carriers without showing any clinical signs.
How the disease spreads
It can be transmitted by direct contact with infected animals, indirectly via fomites, artificial breeding, animal products and by-products, and via vectors. Fomite transmission is a proven method of spread. ASF virus can be spread to other properties via vehicles that have carried infected pigs, clothing and shoes, veterinary instruments (such as needles and buckets), and flies.
Acutely infected pigs shed the virus in high concentrations in all secretions and excretions. Transmission by direct spread generally occurs via the oro-nasal route, but also occurs via the ingestion of waste food containing infected pig products. Pigs that have recovered from ASF can carry the virus for up to 12 months.
Arthropod vectors are also capable of transmitting ASF to pigs. In Africa, the soft-bodied ticks (Ornithodorus spp.) are involved in maintaining a sylvatic cycle between ticks and warthogs. Notably, the predominant form of spread of ASF in the Caucasus appeared to occur via contact and swill feeding, without the need for a sylvatic cycle. In Australia, an Ornithodorus tick (O. gurneyi) is present, but is not known to feed on pigs. Other blood sucking insects, such as mosquitoes and stable flies (Stomoxys spp.), are able to transmit the virus mechanically for 24–48 hours.
Post-mortem and diagnosis
In the peracute and acute forms, the carcass is often in good condition with few lesions. Haemorrages throughout the internal organs (spleen, lymph nodes, kidneys and heart) and the skin are the most common feature.
Lesions associated with the chronic disease are more variable than for the acute form. Lesions may include a non-septic fibrinous pericarditis, interstitial pneumonia, caseous pneumonia, pleural adhesions, lymphadenitis, severe sub-mucosal congestion of the colon with occasional button ulcers of the large intestines, swollen joints, focal areas of skin necrosis and ulcers, and poor body condition.
ASF is clinically indistinguishable from CSF, and both diseases have similar post-mortem lesions. The best way to distinguish between them is by viral isolation on pig leukocyte or bone marrow cultures plus antigen detection in smears or cryostat sections of tissues using a fluorescent antibody test, or the detection of genomic DNA using polymerase chain reaction.
Differential diagnosis
Differential diagnosis includes classical swine fever, erysipelas, salmonellosis, pasteurellosis, pneumonia, Aujeszky’s disease, various poisonings including warfarin, all septic conditions, any cause of ill thrift, any cause of abortion, mummification, stillbirths or weak piglets, mulberry heart disease, thrombocytopenia purpure, and viral encephalitis.
How could the disease enter Australia?
The source of the Georgian outbreak was difficult to determine because of delayed official recognition of the disease. The most likely hypothesis is that ASF entered Georgia from the port of Poti, where pigs gained access to waste containing contaminated pork or pork products from international ships.
Feeding of swill (especially that originating from aircraft and ships) is a major risk factor for the entry of ASF into any country. Australia’s stringent quarantine procedures, including restrictions on pig meat importation, mean that the entry of the disease is unlikely. Possible modes of entry into Australia could include illegally imported pig meat and other pig products, garbage from international aircraft, ships and private vessels, biological products, and illegally imported pigs and boar semen.
Feral pigs could potentially become infected via access to an infected piggery, improperly disposed carcases or waste, improperly disposed garbage dumped by private vessels along the coastline, or contact with insect vectors carrying the virus. If feral pigs became infected with ASF, they would be an important reservoir for the virus and complicate disease control.
Furthermore, the ASF virus is very resistant to environmental conditions. It survives well for many months in raw, unprocessed frozen meat, serum stored at room temperature for 18 months, refrigerated blood for 6 years, and, indefinitely in products stored at -70°C. Heating at 60ºC for 30 minutes will inactivate the virus, but heating at 56°C is ineffective.
Australia has a ban on feeding swill to pigs. Veterinarians that service backyard and peri-urban farms must ensure their clients are informed and aware of the swill feeding ban. Apart from this preventative role, these veterinarians will have important role in the early detection of the virus if it occurred in Australia.
What to do if you suspect African swine fever
ASF is a nationally notifiable disease and early intervention is vital. If you suspect an outbreak, it must be reported to your local government veterinary officer immediately. Alternatively, you can call the free, 24-hour toll-free Emergency Disease Watch Hotline.
The suspected property must be quarantined with no pig, feed, carcass or waste movement off the premises, and movement of people or vehicles on and off the property should be avoided. Suspect pigs should be isolated and appropriate samples taken for testing.
Samples for diagnostic confirmation include:
- whole blood in EDTA for viral testing from live, sick animals
- sera for antibody testing from asymptomatic animals suspected of having subacute or chronic infections
- unpreserved and preserved samples of tonsils, spleen, lymph nodes (gastrohepatic, mesenteric), lung, kidney, liver and ileum from slaughtered pigs and those that have recently died for histopathology and viral testing.
Immediately before autopsy, a range of tissues should be collected and preserved in neutral buffered formalin for histopathology. Blood samples and unpreserved tissues must be chilled and transported to the state or territory diagnostic laboratory. Tissues need to be frozen and forwarded on dry ice if delays are expected.
Early detection and laboratory confirmation of African swine fever is a prerequisite for effective disease control.
Noriel Williams
Animal Health Programs
Biosecurity Services Group
Department of Agriculture Fisheries and Forestry
Further reading
- EMPRES WATCH. African Swine Fever in the Caucasus 2008
 PDF [554kb] (aAccessed 10 July 2009)
PDF [554kb] (aAccessed 10 July 2009) - EMPRES Transboundary Animal Disease Bulletin Issue No. 30. African Swine Fever 2008 PDF [765kb] (accessed 10 June 2009)
- Swiss Agency for Development and Cooperation: Proposal for a control plan for ASF in Georgia 2007 PDF [1.9mb] (accessed 10 July 2009).